What is Congenital Pulmonary Airway Malformation?
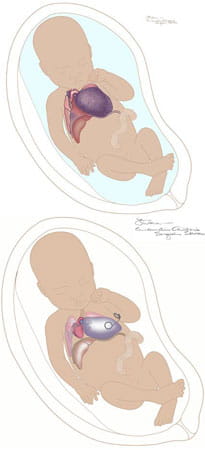
A congenital pulmonary airway malformation (CPAM) is a mass of abnormal fetal lung tissue that forms during pregnancy. This mass, or lesion, is usually located in one lung and it does not function as normal lung tissue.
Lesions vary in size and appearance and can change significantly during the pregnancy. A baby with CPAM can have one lesion or many. These lesions can be solid or filled with fluid.
There is no known cause for CPAM, which was previously referred to as congenital cystic adenomatoid malformation (CCAM). The condition is relatively rare, affecting about 1 in 25,000 pregnancies. It is slightly more common in males than in females. CPAM is not hereditary, so it usually does not recur in families.
Comprehensive, Expert Care for CPAM
At the Cincinnati Children's Fetal Care Center, our experienced maternal and fetal care specialists offer a complete range of diagnostic tests and treatment options for babies with CPAM.
Our team has evaluated more than 400 babies with CPAM since 2004. We know that a diagnosis of CPAM is an emotional experience for families, and in some cases difficult decisions about treatment must be made quickly. At the Fetal Care Center, we are here to help, providing a thorough, compassionate approach to each patient’s care.