What is Spina Bifida?
Spina bifida is a birth defect that occurs when the bones in a baby’s spine do not fully form during early pregnancy. This results in an opening on the back, usually in the mid- to lower back.
Spina bifida is a birth defect that occurs when the bones in a baby’s spine do not fully form during early pregnancy. This results in an opening on the back, usually in the mid- to lower back.
Spina bifida can be mild to severe. The mildest form, called spina bifida occulta, usually does not cause health problems.
The more severe types of spina bifida include myelomeningoceles, meningoceles, lipomyelomeningoceles and other less common lesions.
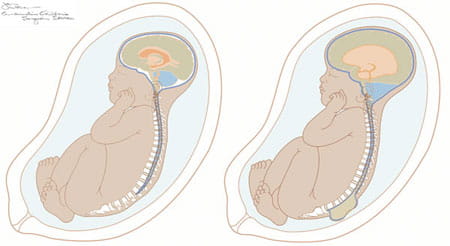
Children who are born with myelomeningocele can experience serious health problems, such as hydrocephalus (an excessive accumulation of fluid in the brain) and paralysis. The severity of paralysis depends on where the opening occurs in the spine.
Some babies who are diagnosed with myelomeningocele during pregnancy may undergo prenatal myelomeningocele surgery to repair the spinal defect.
In fact, results from a seven-year clinical research study called “Management of Myelomeningocele Study (MOMS)” showed that babies who received prenatal repair of myelomeningocele can significantly benefit. The study, published in 2011, compared the effects of fetal surgery vs. surgical repair after birth. It followed 183 women and found that if a baby is operated on while still in the womb, some serious complications of myelomeningocele can be lessened.
MOMS showed that babies who had fetal surgery for myelomeningocele are less likely to suffer from hydrocephalus, a fluid collection in the brain. Babies who are born with hydrocephalus usually need ventriculoperitoneal (VP) shunting, which involves surgically implanting a thin, hollow tube with a valve underneath the skin, behind the ear, that drains excess fluid from the brain into the belly or chest area. In MOMS, 40 percent of babies who had fetal surgery for myelomeningocele needed a VP shunt, while 82 percent of babies who had surgery after they were born needed a VP shunt.
Another finding in the study is that 42 percent of the children who had fetal surgery were able to walk without crutches by age 2½. Only 21 percent of babies who had surgery after birth were able to walk unassisted at that age.
However, all this potential benefit comes at a cost that only the mothers can bear. She must go through extensive surgery, which requires Cesarean deliveries for future pregnancies and a risk for uterine rupture during the current pregnancy. This needs to be discussed with your doctors.
These and other results of MOMS are promising, and physicians are cautiously optimistic. Follow-up studies are under way to assess the long-term effect of prenatal myelomeningocele repair vs. surgery after birth.
Myelomeningocele typically is detected through routine ultrasound during the 18th to 22nd week of pregnancy. A preliminary diagnosis can be made as early as 16 weeks through a blood test that screens for maternal alpha-fetoprotein (AFP). Elevated AFP levels can suggest the presence of a neural tube defect. In this case, patients may undergo an amniocentesis or ultrasound to confirm the diagnosis.
Patients referred to the Cincinnati Children's Fetal Care Center with a diagnosis of fetal myelomeningocele can be seen within a few days of their initial call to the center. We offer a two-day assessment that may include another ultrasound and MRI to confirm the diagnosis and provide additional anatomic detail about the myelomeningocele and the brain. At the end of the second day, patients meet with specialists at the center to discuss the diagnostic findings, treatment options and long-term prognosis. Whether patients can return home after the surgery or need to stay in Cincinnati is also discussed.
Our team includes maternal-fetal medicine specialists, fetal surgeons, pediatric neurosurgeons, neonatologists, genetic counselors, developmental pediatricians and social workers. Referring physicians are welcome to participate in team meetings via video teleconferencing.
Our team works with each family to determine whether fetal surgery is a possible solution. Fetal surgery for myelomeningocele can offer significant benefits to the baby, but it also carries serious risks and potential complications. Our team provides extensive testing and counseling to ensure that patients meet the criteria for fetal myelomeningocele surgery and have all the information they need to make an informed decision about whether to undergo the procedure. Our surgeons have considerable experience in performing this delicate operation. Patients also benefit from exceptional follow-up care before and after the baby is born.
MOMS provides specific guidelines about who is a good candidate for fetal surgery and who is not. The Fetal Care Center follows these guidelines closely.
A partial list includes:
Patients may be eligible for surgery if they meet the following criteria:
Patients are not considered good candidates if the:
Prior to a patient’s first visit, we ask a number of questions by phone to ensure that she meets preliminary criteria for fetal surgery to repair myelomeningocele. An extensive screening takes place during the patient visit to the Fetal Care Center.
Open fetal surgery for myelomeningocele takes place after the 19th week of pregnancy and before the 27th week of pregnancy begins. During surgery, the doctor makes an incision across the mother’s abdomen and opens the uterus. The neurosurgeon removes the myelomeningocele sac, if one is present, and repairs the spinal defect in layers before closing the skin to protect the spinal cord from exposure to amniotic fluid. After the procedure, the uterus and abdomen are closed.
Patients recover in the hospital for four to five days. Weekly follow-up appointments and ultrasound tests take place to monitor the mother’s and baby’s condition.
Women who undergo fetal surgery deliver by a scheduled Cesarean section around 37 weeks gestation (earlier if labor begins before the scheduled date). This is done to prevent any stretching or tearing of the scar that was left on the uterus from the fetal surgery.
When patients are not eligible for fetal surgery or decide against it, surgical repair takes place after the baby is born. This involves operating on the baby within a few days after birth to close the opening in the spine to prevent infection and prevent further injury to the spinal cord and nerves.
However, it cannot correct the defects in the spinal cord and nerves. Babies who are born with hydrocephalus may need a shunt to help drain the excess fluid from the brain. Shunt placement surgery may take place within the first few weeks after the baby’s birth.
Other issues that occasionally can develop in children born with a myelomeningocele include trouble breathing or swallowing. This is called the Chiari II malformation, and it occurs when the myelomeningocele affects a part of the brain called the brainstem.
Learning disabilities, trouble with hand-eye coordination, scoliosis, sexual dysfunction and a number of other problems may develop or become noticeable as the child gets older.
How well a child with myelomeningocele does after fetal surgical repair depends on many factors. Some children will require minimal ongoing care, while others will require medical and educational support for many years.
The Center for Spina Bifida Care at Cincinnati Children’s Hospital Medical Center provides comprehensive, interdisciplinary and family-centered medical care to infants, children and adolescents living with repaired myelomeningoceles and other neural tube defects. In addition to excellence in medical service and care coordination, the center is committed to becoming a leader in spina bifida education and research.
Data based on patients cared for by the Cincinnati Children's Fetal Care Center from Feb. 1, 2004, through June 30, 2023.
For more information or to request an appointment, contact the Cincinnati Children's Fetal Care Center at 1-888-338-2559 or use our online form.
![]()


Myelomeningocele Surgery: Our Biggest and Hardest Decision : Anna Joy is the youngest of four incredible little girls. My pregnancy with her was going smoothly — nothing seemed amiss.
3333 Burnet Avenue, Cincinnati, Ohio 45229-3026
© 1999-2024 Cincinnati Children's Hospital Medical Center. All rights reserved.