What is Inflammatory Bowel Disease (IBD)?
Inflammatory bowel disease (IBD) is an inflammation or swelling in the gastrointestinal tract. There are two main types of IBD: Crohn's disease (CD) and ulcerative colitis (UC). These diseases are not contagious. Sometimes it is hard to distinguish between CD and UC.
Patients are given a diagnosis of IBD-unclassified (IBD-U) until the exact diagnosis is clear. These are life-long conditions that need treatment to prevent future complications. These diseases are not contagious. While these conditions produce similar symptoms and use similar therapies, they are not the same.
How Common Is IBD?
More than three million Americans have IBD. Although children are often diagnosed with IBD during adolescence, IBD can be diagnosed at any age. Boys and girls are both as likely to be diagnosed.
The risk of developing IBD is between five percent to 30 percent if you have a first-degree relative (parent, sibling or child) with the disease. IBD affects people of all ethnic backgrounds.
What Is the Difference between Crohn's and Ulcerative Colitis?
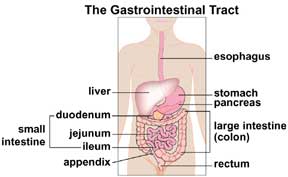
Crohn’s disease can involve any part of the gastrointestinal tract. This includes the mouth to the anus and affects the entire thickness of the intestinal wall. Crohn’s disease mostly affects the last part of the small bowel (ileum) and the colon. People with Crohn’s disease may have inflammation that can ‘skip’ or leave normal areas in between patches of diseased intestine.
Ulcerative colitis affects mainly the colon (the large intestine). It usually involves the rectum and can affect all areas up into the colon. If it affects the whole colon, it is called pancolitis. Ulcerative colitis involves only the lining (first layer) of the bowel (not the entire thickness of the bowel wall). It does not ‘skip’ areas.
Patients with ulcerative colitis and those with Crohn’s disease that involves the colon have a greater risk of getting colon cancer. This risk grows over time if the intestinal tract does not heal with treatment.
What Causes IBD?
We think IBD is caused by a “perfect storm” of exposures to things in the environment. This happens in a person who already has some risk for IBD based on their genes. There is nothing you or your child could have done to prevent getting IBD. The following triggers are thought to play a role in the development of ulcerative colitis and Crohn’s disease:
Possible triggers:
- Genetics (inherited genes): Certain genes you were born with, like family traits, may make it more likely that you will get IBD.
- Environment: Something you are exposed to throughout your life such as food, medications, infections, or toxins. Research has shown that parts of a western diet (highly processed foods) and taking antibiotics multiple times early in life may increase a person’s risk for developing IBD.
- Highly reactive immune system: The patient’s immune system reacts inappropriately. For example, it interprets good bacteria as something harmful and attacks it. This can cause inflammation and lead to the unwanted gastrointestinal symptoms listed below.
- Imbalance of good and bad bacteria: The bacteria that are in the intestine are not balanced.
What Are the Symptoms?
Children with ulcerative colitis and Crohn’s disease have many similar symptoms, including:
- Loose, watery, or frequent bowel movements (diarrhea)
- Blood in bowel movements
- Abdominal (belly) pain
- Decreased appetite
- Weight loss
- Fever
- Fatigue
- Joint pain
- Poor growth
Although some symptoms can be like other illnesses, IBD is a chronic, or long-term condition. It does not resolve on its own.
Ulcerative colitis and Crohn’s disease have times when disease symptoms go away (remission). They also have times when symptoms become more severe (flare). The symptoms, types and severity are unique to every individual. Typically, the symptoms your child had at diagnosis are like the symptoms your child might have during a flare.
How Is IBD Diagnosed?
Because Crohn’s disease and ulcerative colitis share many of the same symptoms, it may be difficult to figure out which condition a child is suffering from. IBD is sometimes mistaken for irritable bowel syndrome (IBD), which also have many of the same symptoms. Diagnosing these diseases requires several tests:
Blood tests to check for conditions like anemia (low hemoglobin), low blood protein (albumin), or evidence of inflammation somewhere in the body (elevated C-reactive protein, sedimentation rate, or white blood cell (WBC) count).
Stool studies to check for infection, blood in the stool, or markers of inflammation in the intestines.
Imaging: special types of abdominal imaging studies such as a CT enterography (CTE) or MR enterography (MRE) to look for inflammation, swelling or narrowing of the intestine. These also look at the areas in the belly outside the intestine for complications of IBD. An MRE has the advantage that it uses magnets, not radiation, to take the pictures.
Upper endoscopy and colonoscopy (looking inside the bowel with a flexible tube and camera) with biopsies to further examine a tissue sample under a microscope. We consider upper endoscopy and colonoscopy as the required test to diagnose IBD.
Capsule endoscopy: swallowing or placing a video capsule during an upper endoscopy to look at the small intestine lining.
How Is IBD Treated?
There are several important goals of treatment including:
- Improving symptoms and maintaining the patient in remission (with little to no symptoms) for long period of time
- Healing the intestine lining and preventing bowel damage or complication
- Restoring normal growth and development
- Restoring quality of life
To reach these goals, we need to think about all aspects of health, such as: diet, medications, and emotional and physical well-being. Most patients require some form of medication. This helps control the swelling and irritation (ulcers) for both ulcerative colitis and Crohn’s disease. There are several types of medications used to control the swelling and irritation. We choose medications based on where the disease is located and the severity of the irritation. In many cases, medications work to control both disease and surgery is not necessary.
Because of the inflammation with IBD, the intestine is unable to do its job of breaking down food and absorbing nutrients. This can cause poor growth, poor weight gain and poor nutrition. Our IBD team includes dietitians who are experts in looking at nutrition. They work with you and your child to create an individual nutrition plan that ensures your child is getting a variety of foods, enough calories, and enough nutrients to support growth and development.
One type of dietary therapy that can be helpful in some patients with Crohn’s disease is Exclusive Enteral Nutrition (EEN) therapy. EEN is a treatment where you get almost all your dietary needs from a nutritional drink or shake. Patients who may a good candidate for EEN will get support from our expert IBD dietitians.
Surgery is an important part of effective treatment for IBD for some patients. Surgery may be recommended when medicine alone cannot control the symptoms, heal the bowel, or reverse bowel damage. Surgery for Crohn’s disease may help get rid of constant symptoms or correct problems. It is not a cure for Crohn’s disease. This is because the intestinal inflammation can return to other parts of the remaining intestinal tract. Ulcerative colitis can be treated by taking out the colon (colectomy) and creating a pouch from the small intestine (J-pouch) so that patients pass stool from their bottom. Cincinnati Children’s is unique for having a group of pediatric colorectal surgeons with special expertise in intestinal and rectal surgery. Surgeons in our Colorectal Center are experienced at performing minimally invasive (laparoscopic) surgeries on children and teens with IBD.
What Are Flares?
Children with IBD can go months or years without having any symptoms. Sometimes symptoms can reappear. This is called a flare. It can happen even when you are working hard to manage your condition through diet and medication.
A flare can involve some or all the symptoms that your child had when they were diagnosed.
How Can Flares Be Managed?
Certain things can trigger a flare, including:
- Not taking medication for IBD as directed
- Taking medications such as antibiotics or NSAIDS (ibuprofen, naproxen, or aspirin)
- Gastrointestinal infection
- Seasonal changes
- Being under a lot of stress, which changes diet and medication adherence, leading to intestinal injury
Your response to a flare can influence the severity of symptoms and how long they last. Following the guidelines below can help:
- Talk to your child’s doctor. Call your child’s doctor at the first sign of serious symptoms. The doctor may recommend blood or stool tests and/or a short course of new medication to treat the flare. The doctor also can help figure out why the flare happened, and if any changes are needed to your child’s treatment plan.
- Help your child stay hydrated, well-rested and active. Hydration is always important for children with IBD, especially for those who are experiencing diarrhea. Offer water and sports drinks with electrolytes (low calorie). Avoid high-sugar drinks such as soda or juice, which can worsen symptoms. Aim for at least 64 ounces of fluid a day.
- Maintain good nutrition. Easy to digest foods can help your child’s bowel recover during a flare (see Sick Day Diet). Your child’s doctor may suggest a nutritional shake during this time.
- Be careful with pain medications. Some over the counter pain medications can make IBD symptoms worse. If your child has joint pain during a flare, try heat therapy, gentle massage, and rest instead of anti-inflammatory medications such as ibuprofen (Motrin, Advil).
- Manage skin irritation and ulcers. If you child has frequent diarrhea during a flare, keep the bottom (anal) area clean and dry. A zinc oxide-based ointment can protect the skin if it is not already broken. If the skin is broken, call your child’s doctor for help.
- Practice good oral hygiene. Flossing and brushing teeth help prevent painful mouth ulcers during a flare. If your child has a mouth ulcer that does not heal in 10 to 14 days, ask the doctor for help.
Long Term Outlook for IBD Patients
No cure is available for IBD. Most children with IBD can control their disease with medication, lifestyle changes and, in some cases, surgery. Our goal is for your child to feel normal and heal the intestine. However, living with IBD is not always easy, especially when symptoms flare. Parents need to be aware of the possible emotional concerns and physical complications that children with IBD face.
Emotional Concerns / Support
A few reasons that children with IBD struggle emotionally are:
- Frustration with the hassles of managing their symptoms
- Not able to maintain a healthy weight because of their symptoms or medications
- Not being like “everyone else”
- Embarrassment about symptoms such as frequent diarrhea
Parents can support their children in several ways. They can help them communicate their feelings and encourage them to participate in all the normal activities or childhood whenever possible. They can also help them find ways to manage these activities with a flare. If emotional concerns persist, a licensed mental health counselor may be able to help.
Our center works closely with our Division of Behavioral Medicine and Clinical Psychology (BMCP). Our psychologists can help families who are adjusting to chronic illness. They can help problem solve some of the trickier situations that may come up due to this new diagnosis of IBD. They can help you and your child understand emotional responses so they can be well managed. Anyone at the early stages of understanding a chronic illness can feel overwhelmed and powerless. They can benefit from learning skills related to managing the illness.
If you have interest in getting extra support and help from a trained mental health professional, talk with your medical team. You can request a referral to the Division of Behavioral Medicine and Clinical Psychology through your nurse and doctor.
Physical Complications
Parents should seek medical attention for their child at the first sign of serious physical complications such as new, severe abdominal pain, worsening blood in the stool, persistent vomiting or vomiting green or brown material, severe fatigue or breathlessness, or unexplained fever. Digestive complications associated with IBD can include:
- Stricture: narrowing of the intestine (scar) that can cause obstruction of the bowel and result in severe nausea, vomiting, or pain after eating.
- Abscess: collection of infected pus in the belly or rectal area.
- Fistulas: abnormal tunnel in the rectal area or between the intestine and other organs.
- Fissures: tears in the anus that cause itching, pain, or bleeding.
- Ulcers in the digestive tract.
- Malnutrition
Non-digestive complications associated with IBD can include:
- Eye inflammation, pain, itchiness, or redness
- Mouth sores
- Joint pain and/or swelling
- Skin sores, bumps, and rashes
- Kidney stones
- Liver disease
These complications could be caused by IBD, by a side effect of your child’s medication or by another, unrelated condition. Early recognition and treatment are very important. Keeping a log of any symptoms your child is having can help you see when a complication may be starting.


