What is Ebstein Anomaly?
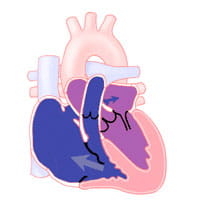
Ebstein anomaly is a defect of the tricuspid valve. The tricuspid valve separates the right atrium (the chamber that receives blood from the body) from the right ventricle (the chamber that pumps blood to the lungs).
Ebstein anomaly is a defect of the tricuspid valve. The tricuspid valve separates the right atrium (the chamber that receives blood from the body) from the right ventricle (the chamber that pumps blood to the lungs).
A chest X-ray will be taken to look at the size of the heart, which may be larger than normal. Often, the diagnosis of Ebstein anomaly is suspected because of the large heart on chest X-ray.
An echocardiogram is used to diagnose Ebstein anomaly. It also helps identify any additional heart defects. This test allows the pediatric cardiologist (heart doctor) to determine the degree of valve displacement, and the severity of valve leakage (insufficiency) or valve narrowing (stenosis). It also helps see the size of the heart chambers, and if a PFO is present.
An electrocardiogram (ECG) records the heart's rhythm. If your child has complained about a racing heart and the answer is not found in this initial test, they may go home with a monitor. Your child may also have an exercise stress test done to better look at their heart function during activity. Some patients with abnormal heart rhythms may need more testing to identify and treat their heart rhythm problems.
Invasive diagnostic testing is not commonly performed today. Certain patients with Ebstein anomaly, may need cardiac catheterization to fully look at their cardiac anatomy and function.

Last Updated 03/2025
Learn more about our editorial policy.
3333 Burnet Avenue, Cincinnati, Ohio 45229-3026
© 2026 Cincinnati Children's Hospital Medical Center. All rights reserved.


