How is Pectus Excavatum Treated?
Younger patients with mild dips can be corrected with a non-surgical vacuum bell treatment. Patients with moderate to severe problems may need surgery. This is not usually done in children younger than age 12 years old. Since children have softer cartilage and more flexible bones than teenagers, the surgery is easier to perform on them and the cosmetic results are better. But now, even young adults are having good outcomes.
Infants and very young children are usually not considered for surgery unless very severe abnormalities or other illnesses require earlier surgery.
What Are The Surgical Procedures for Pectus Excavatum?
Minimally Invasive Surgery (Nuss Procedure)
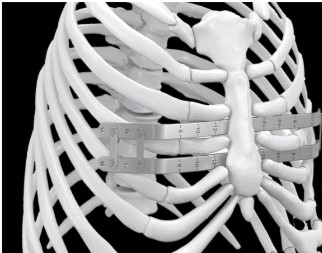
Minimally invasive surgical techniques have been used for more than three decades. With this approach, two small lateral incisions (cuts) are made. A minimum of two bars that have been shaped to the desired chest contour are inserted one at a time into and across the chest below the sternum (breastbone). This is done using an endoscope (instrument used to see the inside of the chest). The bars are held together by bridge connectors that prevent movement of the bars as the chest is reshaped.
Pain Management Options:
Cryoablation:
Cryoablation is a procedure that involves freezing the outer portion of the nerve sheath. This is done while the patient is still under anesthesia and asleep. This makes the area numb longer. It normally takes three months for the outer portion of the nerve to grow back and for the feeling to return. It takes about 24 hours for the cryo to fully take effect.
ES Catheters:
ES catheters are a form of pain management where small catheters are inserted into the muscles of the patient’s back while they are under anesthesia and asleep. The catheters give continuous numbing medication and stay in place for five days. Patients will go home with these catheters and caregivers will be taught how to take them out on day five. The anesthesiologist will call you each day you are home with the catheters to see how your child is doing.
Regardless of which pain management method is used, most patients have the same pain relief by week two to three. Patients may have some residual numbness that doesn’t go away until the bars are removed.



